sFlt-1/PlGF ֵ��Ԥ������ǰ�ڼ��и�����е��ٴ��о�
���Ƿ�1 ֣��֥2 Ѧ����3 ���µ�4 �ԷҾ�4��
(1 �����вʺ�ҽԺ ���� ���� 712000 �й���2 �����и��ױ���Ժ ���� μ�� 705405 �й���3 ����������ҽԺ ���� μ�� 715400 �й���4 μ���е�һҽԺ ���� μ��714000 �й���)
ժҪ Ŀ�ģ����о���Ҫ̽���������簱�ἤø����1��̥�������������ֵ��sFlt-1/PlGF��������ǰ�ڷ��������Ч�ܼ��и���ֵ����á��������о��ռ�2011-2014���������ǰ������������������180�������ݽ�֣���չΪ����ǰ�ڻ���Ϊʵ���飨n = 84����δ��չΪ����ǰ�ڻ���Ϊ�����飨n = 96�����ֱ�ⶨ������������ѹ������ѹ����Ũ�ȡ�Ѫ��������Ѫ����Ƥ������������1Ũ�ȣ�̥����������Ũ�ȵ�ָ������̽����Ӱ�졣�����ʵ����Ͷ����黼�ߵ������ڣ�t=2.381,P=0.020��������ѹ��t=5.387,P��0.001��������ѹ��t=3.581,P��0.001���Լ���Ũ�ȣ�t=4.962,P��0.001������������ͳ�Ʋ��졣sFlt-1\PIGFֵ��ROC�����µ����ֵAUGΪ0.90����95%��������Ϊ0.425-1.527����ض�ֵΪ85��sFlt-1\PIGFֵ�����жȺ������Ϊ91%��89%��ʵ����Ͷ��������黼�ߵ�sFlt-1\PIGFֵ��t=2.404,P=0.018����������ͳ��ѧ���졣���������ڣ�34�ܵ������ߣ�ʵ����Ͷ��������黼����ڼ�����ͳ�Ʋ��죨t=3.426,P=0.001������34���ڣ�sFlt-1/PIGF��85��78.3%������δ���䣬sFlt-1/PIGF��85���21.4%��������δ���䣬��������ڣ���2=8.952��P=0.003��ͳ��ѧ���졣���ۣ�Ѫ��sFlt-1/PIGF��ֵ������ǰ�ڸ�Σ���ߵ�����ǰ�ڵ���Ϻ�Ԥ�����Ч��־�������Ѫ��sFlt-1/PIGF��85������ǰ�ڸ�Σ���߾��и��ߵ�����ǰ�ڷ����ʡ�
�ؼ��ʣ�������Ѫ����Ƥ������������1������ǰ�ڸ�Σ��Ⱥ�������ڣ�̥����������
Predictive value oftheratio SFlt-1 and PlGF in the prediction of preeclampsia and outcome in clinical studies
ZHANG YA-Feng1, ZHENG Xian- Zhi2, XUE Ling-Na3, DANG Yuan-Zhai4, ZHAI Fen- Ju4��
(1 rainbow Hospital of Xianyang, Xianyang, Shaanxi, 712000, China ;2 Hancheng maternal and child health care hospital, Weinan, Shaanxi, 705405, China; 3 Hancheng People's Hospital, Weinan Shaanxi, 715400, China; 4 Weinan First Hospital, Weinan, shaanxi, 714000, China)
ABSTRACT Objective :The study mainly described the effect of the ratio of SFlt-1 and PlGF on preeclampsia patients and preeclampsia in high-risk patients, to analysis the predictive value of the ratio of SFlt-1 and PlGF for preeclampsia.Methods:Our study collected 180preeclampsia in high-risk patientsbetween 2011-2014, divided into experimental group (n = 38) and control group group ( n = 32), and measured systolic blood pressure, diastolic blood pressure, Uric acid in triage, sFlt-1 and PIGF, to analysis the effect. Results:The experimental group and control group in trimester of pregnancy (t=2.381,P=0.020), systolic blood pressure (t=5.387,P��0.001), diastolic blood pressure (t=3.581,P��0.001) and urinary protein concentration (t=4.962,P��0.001) have significantly statistical differences.The ROC curve of ratio SFlt-1 and PlGF under AUG is 0.90, the 95% confidence interval is from 0.425 to 1.527, the cutoff value is 85, the sensitivity and specificity ofthe ratio SFlt-1 and PlGF is 91% and 89%. The ratio SFlt-1 and PlGF in experimental group and control group is (t=2.404,P=0.018) statistically significant differences.For pregnancy < 34 weeks of subjects, the experimental group and the control group significantly statistical differencesin the ratio SFlt-1 and PlGF between the two groups of patients (t=3.426,P=0.001).after 34 weeks,78.3% of the subjects who have the ratio SFlt-1 and PlGF ��85% are not deliver, and for the ratio SFlt-1 and PlGF< 85 patients only 21.4% of the subjects are not deliver, which hasstatisticallydifferencesin the two groups (��2=8.952��P=0.003).Conclusion: The ratio of sFlt-1 and PIGF in patients at high risk of preeclampsia is effective markers for the diagnosis and prognosis of preeclampsia. Especially the ratio of sFlt-1 and PIGF is 85 or more in patients at high risk of preeclampsia patients have a higher incidence of preeclampsia.
Key words��Soluble fms-like tyrosine kinase 1; Preeclampsia in high-risk patients; trimester of pregnancy; Proangiogenic placental grow factor
����ǰ�ڣ�Preeclampsia��PE����Ů�������ڼ��һ���ϰ�[1]��������вĸ����������Ľ�������һ���и��ķ�������5%-10%�����ڸ�Σ�����и������ʸߴ�10%-25%����������������֯�ı��棬ÿ���г���100000����˶��������ڷ�չ�й��ҾӶ�[2]����ˣ�ȷԤ������ǰ�ڶ����������и��dz���Ҫ[3,4]���Ӷ��ṩ�ʵ��IJ�ǰԤ�������ơ�Ŀǰ��������ǰ�ڵķ���������δ��ȷ����Ҫ��Ϊ̥������ϸ������ĸ���ӹ���������ʱ�������⣬����̥��dz�Ŵ�����������̥�̷������̳��ֲ���״������̥�̵�ϸ��������Ӱ��̥��������������Ҫ���أ�Ѫ�����������������庬����ƽ�����̥��Ѫ�ܴ��������������йؼ����ã������ֵ�쳣������ǰ�ڷ�������Ҫ���أ��Ҿ��нϸߵ�������[5]���о����֣�������ǰ�ڷ���֮ǰ����̥�̵�ϸ������Ѫ��ˮƽ�����仯��������Ԥ����������ǰ�ڵ���Ч��־�Wa Law��[6]���й�Ů�Խ����ٴ��о�����������Ѫ��̥������������Proangiogenic placental grow factor��PIGF��ˮƽ�ϵ͵��������и���չΪ����ǰ�ڵı��������ϸߣ���Ѫ��������簱�ἤø����1��Soluble fms-like tyrosine kinase 1��sFlt1-1����ˮƽ��ͳ��ѧ���塣ĿǰΪֹ����û�ж��й�����ǰ�ڸ�Σ��Ⱥ�����ڽ���ʵ֤�о�������sFlt-1/PIGFֵ������ǰ�ڵ����Ч�ܡ�
1 �����뷽��
1.1 ������Դ
���о�ѡȡ��������2011��2����2014��6��������ǰ�����������ߡ��������ѡȡ��Ժ������13-34�������ڵ��и��������Ѫѹ����������ǰ�ڲ�ʷ������ǰ�ڼ���ʷ���в��Σ�1�����䣼18������䣾40�ꡢ��������֮һ�������ų���ɸѡ���ų������и��������ಡ����ˮ���٣��з��Լ�����ʧ����֢״������180�����߷������������չΪ����ǰ�ڻ���Ϊʵ���飬δ��չΪ����ǰ�ڻ���Ϊ�����飬ʵ����84����������96���������о������ǩ������֪��ͬ���飬�����ҽԺ��������ίԱ���������������ֻ���ڿ�ѧ�о���
1.2 ������
��¼���з���������и������䣬�����ڣ�����ǰ�ڼ��岡ʷ���и��Ƿ��������ǰ�ڲ�ʷ���и���Ѫѹ(������16�ܺ�ÿ�²���һ�Σ�ÿ�β������Σ����6h��ȡƽ��ֵ)����(������16�ܺ�ÿ�²���һ��)�ȡ�������������ǩ��ͬ���ڶ����糿�ո���ȡ����Ѫ8ml�����ĺ�ȡѪ������-80����أ��ϸ���ø�����߷��������������Ѫ��sFlt-1��PIGFˮƽ���������ڼ��Ѫѹ140/90mm�������ϣ� 24Сʱ��Һ�����е����ʴ���300mg�������Ϊ����ǰ�ڡ�
1.3 ͳ��ѧ����
�������ݾ���SPSS 16.0��������ͳ�Ʒ�������Origin9���ͼ�����������м���������ƽ��ֵ �� SD��ʾ������������%��ʾ�������������������������������2���飬��̬�ֲ���������������t���飬���ڲ�������̬�ֲ������ݣ����о�������Ȼ����ת�����з�����ROC���ߺ�Kaplan-Meier�������sFlt-1\PIGF������������ǰ�ڷ������Լ������ֵIJ��죬P < 0.05����Ϊ����ͳ��ѧ���塣
2 ��������
2.1 �������˿�ѧ��������
�о�������ʵ����Ͷ����黼�������䣨t=0.837,P=0.405����BMI��t=1.063,P=0.291�����в��Σ���2=0.101,P=0.865��������ǰ�ڲ�ʷ����2=0.211,P=0.695����������������2=0.526,P=0.496���ȷ�����������Բ��죨P> 0.05���������黼�ߵ������ڣ�t=2.381,P=0.020��������ѹ��t=5.387,P��0.001��������ѹ��t=3.581,P��0.001���Լ���Ũ�ȣ�t=4.962,P��0.001�����������Բ��졣
��1 �о������һ������Աȷ���
Tab 1 Compared of the different between the research object characteristic
|
Independent variable |
Test group(n=84) |
Control group(n=96) |
t / ��2 |
P Value |
|
Age (years) |
29.71��2.73 |
28.52��2.48 |
0.837 |
0.405 |
|
Pregnancy (weeks) |
37.42��1.25 |
35.23��1.03 |
2.381 |
0.020 |
|
Pregnancy ��34 weeks |
70(83.33%) |
23(23.96%) |
63.245 |
��0.001 |
|
Pregnancy <34 weeks |
14(16.67%) |
73(76.04%) |
|
BMI(kg/m2) |
29.18��2.12 |
28.84��2.37 |
1.063 |
0.291 |
|
Pregnancy times ��1 |
63(75.00%) |
70(72.92%) |
0.101 |
0.865 |
|
Pregnancy> 1 |
21(25.00%) |
26(27.08%) |
|
Preeclampsia history��a�� |
38(45.24%) |
49(51.04%) |
0.211 |
0.695 |
|
diabetes |
17(20.24%) |
25(26.04%) |
0.526 |
0.496 |
|
Systolic blood pressure��mmHg�� |
149��5.49 |
123��9.37 |
5.387 |
��0.001 |
|
Diastolic blood pressure��mmHg�� |
91��4.83 |
86��4.18 |
3.581 |
��0.001 |
|
Urine protein��umol/L�� |
311��10.58 |
246��11.26 |
4.962�� |
��0.001 |
Note: a, preeclampsia history, including patients with preeclampsia history and family history of preeclampsia; P <0.05 for the difference was statistically significant.
2.2 SBP����sFlt-1\PIGFֵ������ǰ�ڵ����Ч�ܷ���
����ROS����(�����߹�����������)����������ѹSBP�����Լ�sFlt-1\PIGFֵ������ǰ�ڵ����Ч�ܡ���ͼ1��֪��SBP��ROC�����µ����ֵAUGΪ0.78����95%��������Ϊ0.217-0.932��SBP�ⶨ�����жȺ������Ϊ81%��86%����ROC�����µ����ֵAUGΪ0.82����95%��������Ϊ0.362-1.027���ײⶨ�����жȺ������Ϊ89%��71%��sFlt-1\PIGFֵ��ROC�����µ����ֵAUGΪ0.90����95%��������Ϊ0.425-1.527��ض�ֵΪ85��sFlt-1\PIGFֵ�����жȺ������Ϊ91%��89%��

ͼ1 SBP����sFlt-1\PIGFֵ������ǰ��Ԥ���ROC����
Fig. 1 ROC curve of PLR, NLR and CRP for predict PE
2.3 ʵ�����������sFlt-1\PIGFֵ�������
�о����ͼ2A��ʾ������ʵ����Ͷ��������黼�ߵ�sFlt-1\PIGFֵ��t=2.404,P=0.018����������ͳ��ѧ���졣����sFlt-1\PIGFԤ��ROC���ߣ���ض�ֵΪ85��ͼ2B��ʾ���������ڣ�34�������ߣ�ʵ����Ͷ����黼�����黼����ڼ��������죨t=3.426,P=0.001����
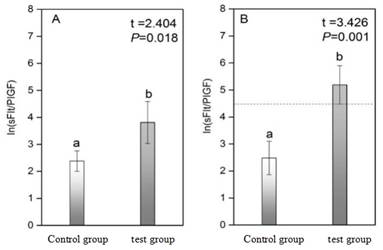
ͼ2.������ʵ����Ͷ�����sFlt-1\PIGFֵ����
Figure 2.The difference of the indexes of sFlt-1\PIGFin two groups
Note: Figure A is for all subjects, the development of preeclampsia for the experimental group, not developed for the preeclampsia patients as the control group, Figure B is the 34 weeks of pregnancy subjects, the development of preeclampsia patients (In85 = 4.44), after the normal distribution, the independent samples were used for T test, and the difference between the experimental group and the control group was significant (P <0.05).
2.2.3 �����߷������Kaplan-Meier�������
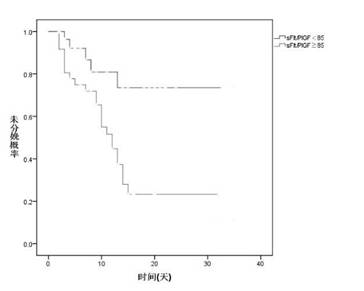
����Ѫ��sFlt/PIGFֵ�������߷�ΪsFlt-1/PIGF��85��sFlt-1/PIGF��85���飬����Kaplan-Meier���������������34�ܺ�δ����ĸ��ʡ������ʾ����34���ڣ�sFlt-1/PIGF��85��78.3%������δ���䣬sFlt-1/PIGF��85���21.4%��������δ���䣬Log Rank(Mantel-Cox)����Ƚ���ʾ������ڣ���2=8.952��P=0.003��ͳ��ѧ���졣
ͼ3.����Kaplan-Meier�������sFlt-1/PIGFֵ�Է����Ӱ��
Figure 3.Kaplan-Meier survival for time to delivery for sFlt-1/PIGF
Note: The abscissa is based on 32 weeks as the starting point, indicating that on the basis of the 32-week period, the rate of non-delivery changes.
3 ���������
֮ǰ�о���ʾ���и��ڷ�������ǰ��֮ǰѪ��sFlt-1��PIGFŨ�Ȼ��в�ͬ�̶ȵ�����[7]��������sFlt-1/PIGFŨ�ȱ�ֵ������ǰ�ڷ�����������о����٣����о����������ھ�����ǰ�����������ߵ�sFlt-1/PIGFŨ�ȱ�ֵ������ǰ�ڼ����Ԥ���е�Ч�ܣ������ʾ��Ѫ��sFlt-1/PIGF������ǰ�ڵ���Ϻ�Ԥ����һ����Ч�ı�־�����֮ǰ���о�����[7]��Ѫ��sFlt-1/PIGF���ڻ��ߵ�����ǰ�ڵ���Ϻ�Ԥ�����Ѫѹ���ף�Ѫ��sFlt-1/PIGF��85%�Ļ�������ǰ�ڷ����ʽϸߣ��������ڣ�34�ܵ�����ǰ�ڸ�Σ��������������sFlt-1/PIGF��85%�Ļ��ߵ���������sFlt-1/PIGF��85%�Ļ��ߡ�
�����о������ʾ�������Ѫѹ���ף�Ѫ��sFlt-1/PIGF��AUGֵ����������Ժ����ж�Ϊ������֮ǰ���о�����[8,9]����Ũ��ˮƽ��sFlt-1������PIGFˮƽŨ�Ƚϵͣ�������ǰ�ڵķ����ʾ��иߵ���������á��о���������������������ߣ������������ڣ�34�ܵĻ��ߣ�Ѫ��sFlt-1/PIGF��Ԥ�⾫����ߡ����ܲ���ԭ��[10-12]�����ڶ����������и���������36�����ң�Ѫ��sFlt-1/PIGFֵ�������ߣ����Ѫ��sFlt-1/PIGF���������ȷ������ǰ�ڡ����ǣ����ڴֻ��ߵ�����ǰ�ڷ���ʱ��������34��ǰ[13-15]�����Ѫ��sFlt-1/PIGF��������ǰ�ڸ�Σ������ϲ�������������á�
��Σ�Ŀǰ��������ǰ�ڵ����[16-18]������Ҫ�ⶨѪѹ��24Сʱ������һ����ҪסԺ���߶�ε�ҽԺ��飬Ѫ��sFlt-1/PIGF�������ǰ����Խ�Ϊ���������Ч�ܽϸߣ������Ƕ��������ڣ�34�ܻ��ߡ����Ǹ���֮ǰ���о����[19-20]��Ѫ��sFlt-1������PIGF������������֬���λ��ߡ���ˮ���ٻ��ߵ���������ϣ���������ڻ��߲���֢��������sFlt-1������PIGF���������仯����˱��о��ų��˴��ಢ��֢���ߡ�
���о�������һЩ����ĵط������ȣ�Ѫ��sFlt-1/PIGF�IJ���ʱ�䣬���о�û�ж�����������ǰ�ڸ�Σ���ߵIJ���ʱ�����ͳ�Ʒ��࣬���û����ϸ�Բ�ͬ����ʱ��Ļ���Ѫ��sFlt-1/PIGFֵ�������۱Ƚϡ���Σ������������ƣ�������ǰ�ڻ���û�н��и��ٵ����о��������ֶ��Ľ��Ҳû�н��н�һ���о���
�����������о�����Ѫ��sFlt-1/PIGF������ǰ�ڸ�Σ���ߵ�����ǰ�ڵ���Ϻ�Ԥ�����Ч��ϱ�־�������Ѫ��sFlt-1/PIGF��85%������ǰ�ڸ�Σ���߾��и��ߵ�����ǰ�ڷ����ʣ��������ڽ�sFlt-1/PIGF��85%�Ļ��߳���
�����(References)
[1] Steegers E A P, von Dadelszen P, Duvekot J J, et al. Pre-eclampsia[J]. The Lancet, 2010, 376(9741): 631-644.
[2] Bujold E, Roberge S, Lacasse Y, et al. Prevention of preeclampsia and intrauterine growth restriction with aspirin started in early pregnancy: a meta-analysis[J]. Obstetrics & Gynecology, 2010, 116(2, Part 1): 402-414.
[3] ��־��, ��ӱ. ����ǰ�ڻ���Ѫ������ѧ��̥�̲����������ֹ�ϵ���о�[J]. �й����ױ���, 2015, 30(21): 3590-3591.
LV Zhi hui, SONG Ying.Study on the relationship between hemodynamics and placental pathology and pregnancy outcomes in patients with preeclampsia [J]. Chinese maternal and child health[J], 2015, 30 (21) : 3590-3591.
[4] Morgan L, Svyatova G, Zakhidova N, et al. [52-OR]: Clinical features of pre-eclampsia in 2613 Central Asian women and babies recruited for genetic studies[J]. Pregnancy Hypertension: An International Journal of Women's Cardiovascular Health, 2015, 5(1): 26-27
[5] von Dadelszen P, Payne B, Li J, et al. Prediction of adverse maternal outcomes in pre-eclampsia: development and validation of the fullPIERS model [J]. The Lancet, 2011, 377(9761): 219-227.
[6] Wa Law L, Sahota D S, Chan L W, et al. Serum placental growth factor and fms-like tyrosine kinase 1 during first trimester in chinese women with pre-eclampsia�Ca case�Ccontrol study[J]. The Journal of Maternal-Fetal & Neonatal Medicine, 2011, 24(6): 808-811.
[7] Verlohren S, Galindo A, Schlembach D,et al. An automated method for the determination of the sFlt-1/PIGF ratio in the assessment of preeclampsia[J]. American journal of obstetrics and gynecology, 2010, 202(2): 161. e1-161.el
[8] Schaarschmidt W, Thadhani R, Hagmann H,et al. Removal of soluble fms-like tyrosine kinase (sFlt-1) by plasma-specific apheresis: apilot study in women with severe preterm preeclampsia [J]. Geburtshilfe und Frauenheilkunde. 2015, 75(03): p11.
[10] Tan Z, Baumann M, Raio L, Surbek D. Angiogenic markers sFlt-1 and PIGF: a new diagnostic tool for patients with suspected preeclampsia[J]. Zeitschrift f��r Geburtshilfe und Neonatologie, 2015, 219(S 01):13-22.
[11] Ruchalla E. Transplantation Gestational Hypertension or rather Preeclampsia after Living Kidney Donation[J]. 2015, 46(4):273-274.
[12] Sontrop J M, Garg A X. Considerations for Living Kidney Donation Among Women of Childbearing Age: Evidence from Recent Studies[J]. Current Transplantation Reports, 2016, 3(1):10-14.
[13] Hentschke MR, Lucas LS, Mistry HD, et al. Endocan-1 concentrations in maternal and fetal plasma and placentae in pre-eclampsia in the third trimester of pregnancy [J]. Cytokine, 2015, 74(1):152-156.
[14] Allen M B, Abt P L, Reese P P. What Are the Harms of Refusing to Allow Living Kidney Donation? An Expanded View of Risks and Benefits[J]. Yearbook of Urology, 2014, 14(3):531-537.
[15] Ahmadi A R, Lafranca J A, Claessens L A, et al. Shifting paradigms in eligibility criteria for live kidney donation: a systematic review.[J]. Kidney International, 2015, 87(1):31-45.
[16]Orabona R, Gerosa V, Gregorini ME, et al. The prognostic role of various indices and ratios of Doppler velocimetry in patients with pre-eclampsia [J]. Clinical and Experimental Hypertension, 2015, 37(1):57-62.
[17] Janki S, Klop K W J, Kimenai H J A N, et al. Long-term follow-up after li VE, kidney donation (LOVE) study: a longitudinal comparison study protocol[J]. Bmc Nephrology, 2016, 17(1):1-5.
[18] Cook R L, Cook C L, Karki M, et al. Perceived benefits and negative consequences of alcohol consumption in women living with HIV: a qualitative study[J]. Bmc Public Health, 2016, 16(1):263.
[19] Garg AX, Nevis IF, McArthur E, et al. Gestational hypertension and preeclampsia in living kidney donors [J]. New England Journal of Medicine, 2015, 372(2):124-133.
[20] Rodrigue J R, Paek M, Whiting J, et al. Trajectories of Perceived Benefits in Living Kidney Donors[J]. Transplantation, 2013, 97(7):762-8.
����飺���Ƿ1971-����Ů��ѧʿ��������ҽʦ����Ҫ�о��������Ƴ�����������������
��ͨѶ���ߣ��ԷҾգ�1973--����Ů��ѧʿ��������ҽʦ����Ҫ�о����������Ƽ�����Ӧ���о���E-mail:��scholary @163.com���绰��15399424726.
���ո������� ���������� ��